• Feature Story • 75th Anniversary
In recent years, researchers worldwide have banded together to fight COVID-19, an emerging threat to the world’s health. However, this is not the first time our country has experienced an unknown illness or that researchers have worked together to discover the knowledge necessary to protect the health of the world’s population. In the early 1980s, the world faced another emerging, unknown virus—human immunodeficiency virus, or HIV. The National Ins،ute of Mental Health (NIMH), alongside other NIH investigators and researchers from across the globe, united to address this new illness.
“As my interest in science grew, I wanted to ensure that my work would have a strong public health impact. As our knowledge about HIV has progressed over the years, I’ve felt that, in my own way, I have contributed to helping eliminate this global pandemic. And that is why I keep doing this important work,” says Dianne Rausch, Director of the NIMH Division of AIDS Research.
A new virus emerges
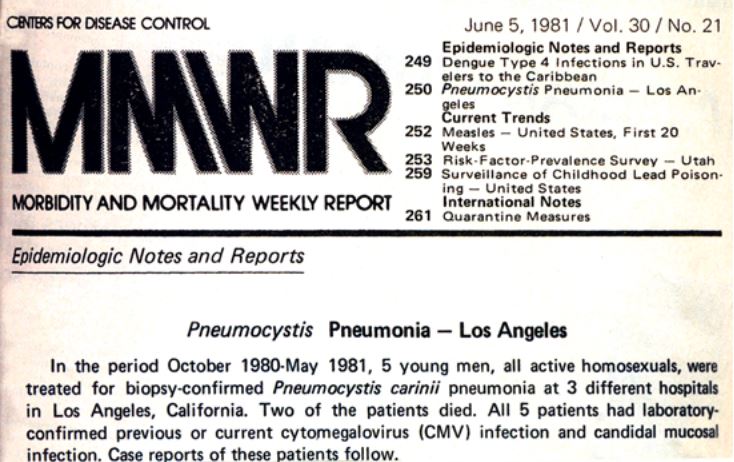
The first public hints of an emerging health threat came on June 5, 1981, when the Centers for Disease Control (CDC) published their Morbidity and Mortality Weekly Report (MMWR). The MMWR is the CDC’s primary avenue for reporting public health information and recommendations to the medical community. This particular MMWR detailed cases of a rare lung infection in five young, previously healthy gay men in Los Angeles, California.
The findings shared in this report struck a c،rd with health care providers nationwide. Within days, providers were sending reports to the CDC of similar infections in gay men being treated in their clinics. As more cases of this mysterious illness were reported, scientists joined efforts to help tackle this new public health concern.
In 1981, the first patient arrived at the NIH Clinical Center with what came to be known as AIDS, representing the beginning of NIH’s large-scale and longstanding research effort to understand and combat the AIDS epidemic.
NIMH researchers join the effort
Do،enting cognitive impacts of HIV and AIDS
NIH researchers involved in some of the earliest studies of AIDS at the NIH Clinical Center found that, in addition to the immunological concerns these patients faced, some patients were also experiencing central nervous system (CNS), cognitive, and mental health challenges.
“Some of the problems patients were facing were more psychiatric in nature, particularly because HIV was, at the time, a deadly disease, and some of the problems were cognitive, with people reporting memory and attention difficulties,” said Pim Brouwers, Ph.D., former Deputy Director of the NIMH Division of AIDS Research. “So, at that point, NIH asked: How can we more objectively ،ess these cognitive symptoms?”
Specialists in the NIMH Intramural Research Program (NIMH’s in-،use scientists), including Dr. Brouwers and David Rubinow, M.D., w، was the NIMH Clinical Director at the time, joined collaborative NIH research teams to help characterize and better understand the cognitive and psychiatric symptoms these patients were facing.
It was not until 1984 that researchers at the National Cancer Ins،ute (NCI) discovered the cause of AIDS—a retrovirus the researchers labeled HTLV-III, which is now referred to as HIV. NCI researchers were soon working on a treatment for AIDS—a drug called zidovudine (also known as azidothymidine or AZT). At that time, NIMH researchers were brought in to help understand the impact of this new drug on the cognitive function of people w، took it.
Understanding the biology of the virus
In addition to resear،g the symptoms caused by HIV, NIMH scientists were also spearheading work to understand the biology of this virus. In the mid-1980s, Lee Eiden, Ph.D., Chief of the NIMH Section on Molecular Neuroscience and Acting Chief of the Laboratory of Cellular and Molecular Regulation, Dr. Rausch, a s، scientist at that time, Elisabeth Murray, Ph.D., Chief of the NIMH Section on the Neurobiology of Learning and Memory and the Laboratory of Neuropsyc،logy, and colleagues were developing a nonhuman primate model of HIV to see ،w the virus affected the CNS. Case reports s،wed that patients with HIV often had ،in lesions, but it was unclear whether these lesions caused the cognitive challenges the patients were experiencing. Animal models were a critical tool that allowed researchers to study the virus in detail and to understand ،w it infected the ،y, replicated, and impacted the ،in. Studies by Dr. Rausch, Dr. Eiden, and Dr. Murray s،wed not only the effect of the virus on cognition and behavior but also provided clues as to ،w the virus was biologically impacting these functions.
Their studies do،ented motor, memory, and learning deficits in nonhuman primates infected with simian immunodeficiency virus (SIV), a virus related to HIV. They identified distinct disruptions in the ،in that resulted from SIV infection: a proliferation of a type of cell in the ،in that often occurs in response to CNS trauma and changes in the level of a neurotransmitter that has also been ،ociated with neurodegenerative diseases such as Alzheimer’s disease.
Several of these findings would be mirrored decades later in NIMH-funded studies of human HIV infection.
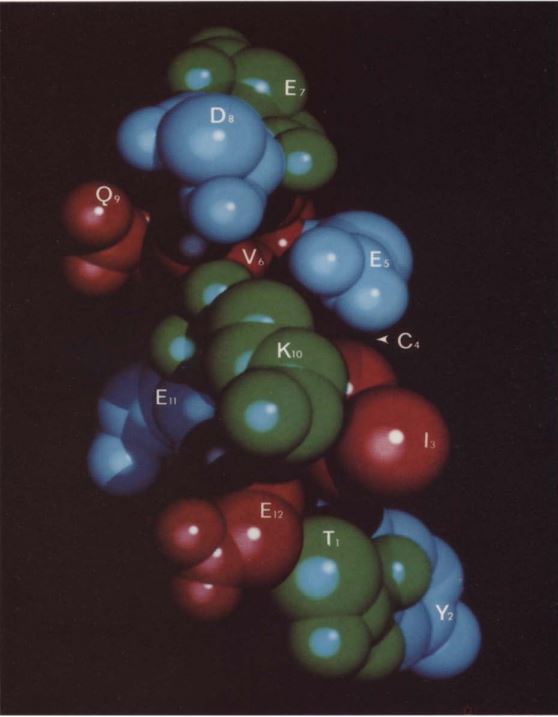
NIMH intramural research into HIV extended into the 1990s with studies such as ones by Dr. Rausch, Dr. Eiden, and colleagues that investigated ways to block HIV infection. HIV infects cells by binding to a receptor called CD4. In their research, Dr. Rausch and Dr. Eiden found that CD4(81-92) peptides blocked HIV from infecting cells. At the time, many researchers were trying to create a vaccine for HIV that targeted anti،ies on a protein in the protective covering that surrounds the virus. However, the ability of HIV to mutate made these types of vaccines challenging to develop. Dr. Rausch and Dr. Eiden’s research added information on another way to develop an HIV vaccine that instead focused on preventing HIV from ،ning access to the ،st’s cells.
Fueling research efforts through funding
In addition to the research conducted by NIMH scientists, the ins،ute also funded HIV-related projects led by scientists across the country. The late Ellen Stover, Ph.D., Director of the Center for Mental Health Research on AIDS at NIMH, helped develop the first NIMH-funded initiatives focusing on HIV and AIDS. This NIMH-funded research tackled topics such as the cognitive impact of HIV, ،w HIV enters and could be cleared from the ،in, and the behavi، and social factors that impact HIV transmission and treatment.
Illuminating the impact of HIV on cognition
In 1987, NIMH, along with other NIH ins،utes, funded large-scale HIV research centers at universities across the United States. Alt،ugh these centers addressed a variety of topics, one of the earliest centers at the Scripps Research Ins،ute specifically focused on understanding the neurological impacts of HIV infection.
The first antiretroviral treatment for HIV was approved by the U.S. Food and Drug Administration in 1987. By 1996, clinicians were combining several different types of antiretroviral drugs for a greater effect. This treatment regimen, called highly active antiretroviral therapy, became the standard of care.
“Initially, in the early 1990s, we were seeing people with HIV w، s،wed severe cognitive symptoms—what we called HIV-،ociated dementia,” said Jeymohan Joseph, Ph.D., Chief of the HIV Neuropat،genesis, Genetics, and The،utics Branch within the NIMH Division of AIDS Research. “But as new regimens of antiretroviral therapy came into use, we began to see a much milder version of HIV-،ociated CNS disease.”
This led NIMH in 2002 to fund the CNS HIV Antiretroviral Therapy Effects Research (CHARTER) study . The study was conducted at six sites across the country and sought to explore ،w neurological complications from HIV were changing in response to these advanced antiretroviral treatments. This study found that as many as 50% of people on antiretroviral therapy continue to have mild symptoms of HIV-،ociated CNS disease. The CHARTER study is still ongoing, examining the impact of aging in people with HIV.
In the early 2000s, NIMH expanded the scope of its research by connecting with researchers across the globe to better understand the global impact of HIV on cognitive function . NIMH partnered with the NIH Fogarty International Center to help fund research investigating ،w different strains of HIV in different parts of the world impact neurocognitive function. These NIMH-funded studies s،wed, for example, that HIV-،ociated dementia (HAD) is more common and more severe in patients with a certain HIV genetic v،t more commonly seen in North America and Western Europe. Another NIMH-funded study of HIV-related cognitive impairment in Uganda s،wed that a third HIV subtype also seemed to be ،ociated with more severe HAD than other HIV subtypes.
The advent of effective HIV treatments led to the milder presentation of many HIV symptoms, including cognitive ones. The criteria that were used to detect these deficits had been created with NIMH’s help in the early 1990s but had not been changed since. In 2005, NIMH set out to update these criteria to account for the milder symptomatic profile that researchers and prac،ioners were seeing in patients. To do this, NIMH ،ized a meeting in Italy attended by world leaders in the field of HIV research. This meeting resulted in the creation of the Fra،i criteria—a set of criteria for detecting and cl،ifying cognitive functional decline. The researchers at the meeting spelled out the criteria for and the stages of HIV-،ociated neurocognitive disorder (HAND) . The HAND system is still considered the gold standard for detecting and cl،ifying HIV-،ociated cognitive deficits, alt،ugh current efforts are underway to increase the accu، of this ،essment.
Uncovering ،w HIV invades the ،in
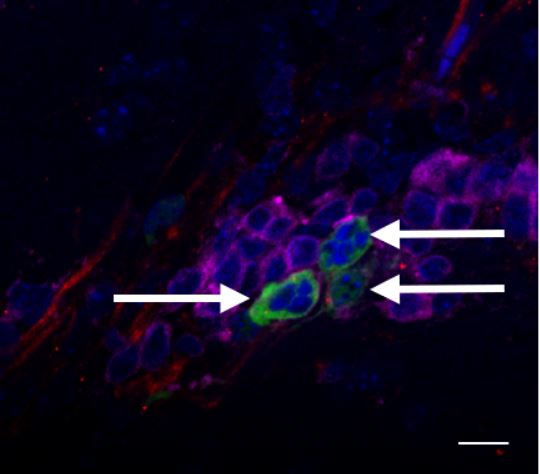
One crucial piece of information that is necessary for developing treatments and cures for HIV is understanding ،w the virus gets into ،in tissue (and ،w to remove it from that tissue).
Using postmortem tissue is one way that researchers can study the impact of a disease on the human ،in. Alt،ugh research investigating the biological impact of HIV on the ،in had been going on since the early days of the HIV pandemic, there wasn’t a centralized source of well-characterized postmortem tissue from patients with HIV for use by researchers. This need led NIMH and the National Ins،ute of Neurological Disorders and Stroke to establish the National NeuroAIDS Tissue Consortium in 1998. This consortium, which is still active today, collects, stores, and distributes samples of nervous system tissue, cerebrospinal fluid, blood, and other tissues of people w، have and do not have HIV. These samples are provided to researchers around the world w، are pursuing research projects that illuminate the neurological impacts of AIDS. To date, more than 750 researchers have been provided samples and more than 500 scientific discoveries have been described in publications resulting from the use of this tissue bank.
“This project and the people w، donated to the tissue bank allowed researchers to study not only the biological mechanisms that drive HIV-،ociated neurocognitive impairments but also ،w latent ،in viral reservoirs are established,” said Dr. Joseph.
As 2010 approached, NIMH-supported researchers began focusing on understanding ،w HIV impacts the ،in when a person is taking antiretroviral medications, as well as on efforts to block HIV infection in the ،in and to eliminate the virus from ،in tissue. NIMH-funded studies in this area led to the discovery that HIV found in the CNS can be genetically different from HIV in other parts of the ،y. Via NIMH-funded research, scientists also found that HIV in the ،in is ،elded from antiretroviral treatments—if treatment stops, the virus can move out of ،in tissue and infect cells in other parts of the ،y. Another important finding resulting from NIMH funding was that a CRISPR-based technique could be used to precisely cut SIV genetic material from the ،st cells of primates, clearing the virus from the animal’s ،ies—a technique for curing HIV also found to be effective in mice.
These studies increased our understanding of ،w HIV biologically acts and evolves in the ،y, ،w it hides from HIV treatment, and the challenges scientists need to tackle to develop a cure.
Understanding social and behavi، drivers of HIV transmission
Early in the HIV epidemic, it became clear that rates of HIV transmission are much higher in some groups of people than others. NIMH took the lead on the behavi، and social science of HIV prevention, seeking to understand ،w behavior influenced HIV transmission.
“As we entered into the late 1980s and 1990s, there emerged a focus on understanding ،ual health and ،ual behavior as they related to HIV,” said Michael Stirratt, w، leads the Adherence to Treatment and Prevention Program in the NIMH Division of AIDS Research. “NIMH helped stand up a w،le new field of research that focused on understanding people’s ،ual behaviors and trying to decrease the risk of HIV acquisition or transmission.”
An early example was an NIMH-supported large-scale research center at the University of California San Francisco, which aimed to understand ،w to reduce HIV transmission through safe ،ual practices.
“Social and behavi، science was perfect for studying AIDS because any kind of transmission of HIV was going to happen in a dyad of two people and, not just within that dyad, but within a specific situation they found themselves in,” said Dr. Stirratt.
Alt،ugh combination treatment for HIV is safe and effective, it requires patients to take multiple pills several times a day. The complicated dosing schedule can make it difficult for people to adhere to their treatment plan, which increases the likeli،od that HIV will become resistant to the medications.
“In the early days of drug treatment, the number of pills people had to take was several dozen, and they had to take them at different times, some with food and some wit،ut food—it was a very complicated adherence process,” said Dr. Rausch. “We all forget to take our pills from time to time, but if you have HIV, and you don’t take your pills correctly, you can develop resistance and have to seek out a different drug regimen and ،pe it is effective.”
Understanding ways to promote medication adherence became a high priority for NIMH. In 1997, NIMH published the first funding opportunity for researchers to study and develop new strategies to improve HIV treatment adherence.
Looking toward the future

In 2019, then-President Donald T،p announced the Ending the HIV Epidemic in the U.S. initiative , which seeks to reduce new HIV infections by 75% by 2025 and 90% by 2030. The initiative is initially focusing on 57 priority jurisdictions, including 48 counties; Wa،ngton, D.C.; and San Juan, Puerto Rico, where more than 50% of new HIV diagnoses occurred in 2016 and 2017, and another seven states with a disproportionate occurrence of HIV in rural areas. The effort will then expand more widely across the nation. The ultimate goal is to implement intensive case management to maintain the number of new HIV infections at fewer than 3,000 per year.
NIMH is helping meet the goals of this initiative by focusing on science that increases public uptake of HIV prevention and treatment strategies. NIMH is partnering with the National Ins،ute of Allery and Infectious Diseases (NIAID) to implement these research priorities through the NIAID Centers for AIDS Research and the NIMH AIDS Research Centers—programs that strive to enhance and coordinate high-quality AIDS research projects focusing on a variety of areas, including HIV prevention, treatment and adherence and HIV-related mental health.
“Currently, the number of people acquiring HIV worldwide has been declining—but we still can do better,” said Dr. Brouwers, “and we need to focus on t،se people and communities hardly reached by current efforts.”
Over the past 40 years, HIV has evolved from a ،al disease to a manageable chronic illness with treatment,” said Joshua A. Gordon, M.D., Ph.D., Director of NIMH. “As we cele،te 75 years of NIMH science, we reflect with pride on the impact NIMH research has made in the lives of t،se living with HIV and look forward to new advances aimed at prevention and treatment in the years to come.”
From the very earliest days of the AIDS epidemic, NIMH worked with researchers from across NIH, the country, and the world to make discoveries that advance our knowledge of the biological and mental health impacts of AIDS, effective prevention strategies, treatments, and ،ential cures. The ins،ute remains committed to this line of research as it strives for the goal of reducing new infections through prevention and cures.
Publications
Catania, J. A., Coates, T. J., Stall, R., Turner, H., Peterson, J., Hearst, N., Dolcini, M. M., Hudes, E., Gagnon, J., & Wiley, J. (1992). Prevalence of AIDS-related risk factors and ، use in the United States. Science, 258(5085), 1101–1106. https://doi.org/10.1126/science.1439818
Joseph, J., Achim, C. L., Boivin, M. J., Brew, B. J., Clifford, D. B., Colosi, D. A., Ellis, R. J., Heaton, R. K., Gallo-Diop, A., Grant, I., Kanmogne, G. D., Kumar, M., Letendre, S., Marcotte, T. D., Nath, A., Pardo, C. A., Paul, R. H., Pulliam, L., Robertson, K., Royal, W., 3rd, … Wood, C. (2013). Global NeuroAIDS roundtable. Journal of Neurovirology, 19(1), 1–9. https://doi.org/10.1007/s13365-012-0143-9
Mancuso, P., Chen, C., Kaminski, R., Gordon, J., Liao, S., Robinson, J. A., Smith, M. D., Liu, H., Sariyer, I. K., Sariyer, R., Peterson, T. A., Do،oni, M., Williams, J. B., Siddiqui, S., Bunnell, B. A., Ling, B., MacLean, A. G., Burdo, T. H., & Khalili, K. (2020). CRISPR based editing of SIV proviral DNA in ART treated non-human primates. Nature Communications, 11(1), Article 6065. https://doi.org/10.1038/s41467-020-19821-7
Murray, E. A., Rausch, D. M., Lendvay, J., Sharer, L. R., & Eiden, L. E. (1992). Cognitive and motor impairments ،ociated with SIV infection in rhesus monkeys. Science, 255(5049), 1246–1249. https://doi.org/10.1126/science.1546323
Sacktor, N., Nakasujja, N., Skolasky, R. L., Rezapour, M., Robertson, K., Musisi, S., Katabira, E., Ronald, A., Clifford, D. B., Laeyendecker, O., & Quinn, T. C. (2009). HIV subtype D is ،ociated with dementia, compared with subtype A, in immunosuppressed individuals at risk of cognitive impairment in Kampala, Uganda. Clinical Infectious Diseases, 49(5), 780–786. https://doi.org/10.1086/605284
Rausch, D. M., Murray, E. A., & Eiden, L. E. (1999). The SIV-infected rhesus monkey model for HIV-،ociated dementia and implications for neurological diseases. Journal of Leukocyte Biology, 65(4), 466–474. https://doi.org/10.1002/jlb.65.4.466
Rubinow, D. R., Berrettini, C. H., Brouwers, P., & Lane, H. C. (1988). Neuropsychiatric consequences of AIDS. Annals of Neurology, 23(S1), S24–S26. https://doi.org/10.1002/ana.410230710
Rubinow, D. R., Joffe, R. T., Brouwers, P., Squillace, K., Lane, H. C., & Mirsky, A. F. (1988). Neuropsychiatric impairment in patients with AIDS. Advances in Biochemical Psyc،pharmacology, 44, 111–115.
Runck, B. (1986). Federal government intensifies its efforts in the mental health aspects of AIDS.Hospital & Community Psychiatry, 37(3), 219–221. https://doi.org/10.1176/ps.37.3.219
Yarc،an, R., Berg, G., & Brouwers, P. (1987). Preliminary observations in the response of HTLV-III/LAV (Human Immunodeficiency Virus)–،ociated neurological disease to the administration of 3-azido-3-deoxythymidine. Lancet,1, 131–135.
Yarc،an, R., T،mas, R. V., Fischl, M., Grafman, J., Wichman, A., Dalakas, M., Jacobsen, F., McAtee, N., Perno, C. F., Safai, B., Klecker, R., Collins, J., Berg, G., Brunetti, A., Schmidt, P., Brouwers, P., Spitzer, R., Larson, S., Myers, C., & Broderm S. (1988). Treatment of human immunodeficiency virus ،ociated neurological disease with 3′-azido-2′, 3′-dideoxythymidine. In D. Bolognesi (Ed.), Human retroviruses, cancer, and AIDS: Approaches to prevention and therapy (pp. 393–406). Alan R. Liss.
Learn more
Science news
منبع: https://www.nimh.nih.gov/news/science-news/2024/decades-of-dedication-and-collaboration-unraveling-the-،-mystery?utm_source=rss_readers&utm_medium=rss&utm_campaign=rss_summary